
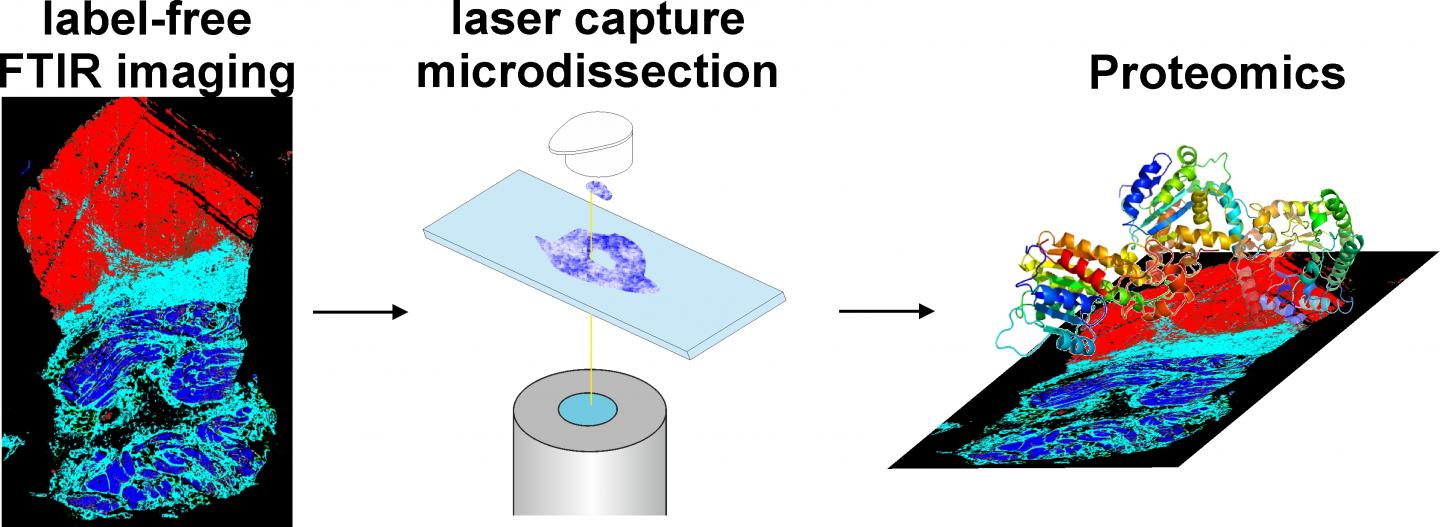
IMAGE: Label-free Fourier transform infrared (FTIR) imaging (left) classifies the unaltered tissue thin section (red: tumor, cyan: connective tissue, blue: muscle). This information is then used to cut out tissue samples… view more
Credit: American Journal of Pathology
Philadelphia, PA, February 12, 2019 – Label-free digital pathology using infrared (IR) imaging with subsequent proteomic analysis for bladder cancer (BC) has revealed the first protein biomarker (AHNAK2) for BC. AHNAK2 differentiates between chronic cystitis (inflammation of the bladder) and a non-muscle invasive-type BC (carcinoma in situ) which is challenging to diagnose. A report in the American Journal of Pathology describes this new diagnostic procedure, which is label-free, automated, observer-independent, and as sensitive and specific as established histopathological methods.
Distinguishing benign inflammatory conditions in the bladder from low-grade and advanced cancers can be difficult, especially since some BC treatments induce inflammation.
“We developed this label-free digital pathology annotation system by IR imaging to support the pathologist, similar to driver assistance in cars. This technique in combination with a proteomics approach allowed us to identify AHNAK2 as an important new biomarker for BC, and the results encourage us to transfer this label-free digital technique to other pathologies,” explained Klaus Gerwert, PhD, Chairman of the Department of Biophysics and the PURE (Protein Research Unit Ruhr within Europe) consortium at Ruhr University Bochum, Germany.
Using label-free Fourier transform IR (FTIR) imaging, investigators were able to classify unaltered tissue thin sections by color to identify regions of interest. “The resulting index color images automates tissue classification, including cancer type, subtype, tissue type, inflammation status, and even tumor grading,” noted Prof. Dr. Gerwert.
In an analysis of 103 freshly-frozen samples that included confirmed diagnoses for 41 cystitis, 19 low-grade carcinoma, and 43 high-grade carcinoma, FTIR imaging showed a specificity of 95 percent, sensitivity of 95 percent, and an accuracy of 95 percent compared to stained images reviewed by a trained pathologist. The technique also differentiated cancerous from healthy tissue as well as low- from high-grade carcinoma.
Laser capture microdissection was then used to obtain homogenous tissue samples for protein analysis by proteomics. By comparing tissue from patients with inflammatory bladder (cystitis) to samples from patients with invasive, high-grade urothelial carcinoma, the investigators identified three potential biomarkers, with the protein AHNAK2 found to be the best performing candidate biomarker.
In a large cohort that included 310 freshly-frozen, paraffin-embedded tissue samples (51 high-grade cancers, 67 carcinoma in situ [CIS], 84 low-grade cancers, and 108 patients with severe cystitis), AHNAK2 measurement achieved 97 percent sensitivity and 69 percent specificity in differentiating between severe cystitis with reactive urothelial atypia (RUA) vs CIS. It also displayed high sensitivity in distinguishing low versus invasive high grades and low grades vs CIS.
“In our study, AHNAK2 was identified and verified in two steps as a candidate biomarker for BC,” said Barbara Sitek, PhD, Deputy Director, Medizinisches Proteom-Center (MPC), Ruhr University, Bochum, Germany. “AHNAK2 has already been proposed as a potential prognostic biomarker for clear renal cell and pancreatic cancers and is part of a urinary mRNA panel for the diagnosis of BC and prediction of tumor aggressiveness.”
The investigators believe AHNAK2 could be a very helpful tool for detecting CIS recurrence or persistence, particularly because misdiagnosis of CIS can delay treatment of an aggressive malignancy or could lead to unnecessary treatment or bladder removal.
BC is the second most common urogenital malignancy, with about 430,000 new cases diagnosed worldwide in 2012. About 75 percent of newly diagnosed patients have non-muscle invasive, mostly low-grade BC, and about 25 percent have high-grade BC at the stage of infiltration of smooth muscle. The presence of acute or chronic inflammation (urocystitis) with RUA can complicate diagnosis, especially when patients with BC have been purposely treated with pro-inflammatory agents. The current gold standard for tumor grading and staging of BC is the visual inspection of stained tissue thin sections by a pathologist; immunohistochemistry is also used but can be difficult to interpret.
###
Disclaimer: AAAS and EurekAlert! are not responsible for the accuracy of news releases posted to EurekAlert! by contributing institutions or for the use of any information through the EurekAlert system.